

Abstract
Introduction: Venous thromboembolism (VTE) is a common complication of cancer, associated with significant morbidity and mortality. Low-molecular weight heparin (LMWH), the most widely used anticoagulant in this setting, is expensive and burdensome. Rivaroxaban (Riva) was approved for treatment of VTE in 2012, but there is limited experience in cancer-associated thrombosis (CAT). In 2014, we established a Clinical Pathway (CP) to guide use of rivaroxaban (Riva) for CAT at Memorial Sloan Kettering Cancer Center. We were concerned that a direct oral anticoagulant (DOAC) would be more likely than LMWH to cause upper gastrointestinal (GI) bleeding in the presence of abnormal mucosa. DOACs have partial renal clearance and are active in the urine, in contrast to LMWH, and we also anticipated increased genitourinary (GU) tract bleeding in the presence of GU lesions. Therefore, the key to our CP has been to recommend against use of Riva or other DOAC in the setting of active (GI) or (GU) tract lesions. As the elderly are known to be at higher risk of bleeding from anticoagulation, the CP recommended reduced dose Riva in patients≥75 year old (yo), (10 mg bid X 3 wks., followed by 15 mg daily). Otherwise, we adhere to the standard FDA approved guidelines. We published a 200-patient cohort in 2016 demonstrating rates of recurrent VTE and bleeding that were at least as low as historical controls with LMWH.
This past year, two randomized clinical trials were published comparing a DOAC with dalteparin ("Hokusai VTE Cancer" of edoxaban, Raskob G.E. et al, NEJM, 2017, and "Select-D" of Riva, Young A.M. et al, JCO 2018). Both studies showed a trend towards better efficacy with the DOAC, but with increased GI/GU bleeding. However, those studies did not exclude patients with known GI/GU lesions. We now report our expanded experience with Riva treatment of CAT, confirming the safety and efficacy of Riva treatment of CAT when guided by our CP.
Methods: From 1/1/2014 through 10/31/2016, 2000 patients at MSKCC received Riva. 1072 had CAT, defined as a lower extremity DVT and/or PE in a patient with active cancer or receiving cancer therapy. (The other 928 patients did not have active cancer, or received Riva for other indication). All patients treated with Riva for CAT are included in this analysis, even in the presence of active GI/GU lesions. Recurrent VTE, major bleeding (MB), clinically relevant non-major bleeding (CRNMB) leading to discontinuation of Riva, and death were competing risk endpoints for the purpose of the analysis. We also evaluated the outcomes of the subgroup of patients ≥75 yo.
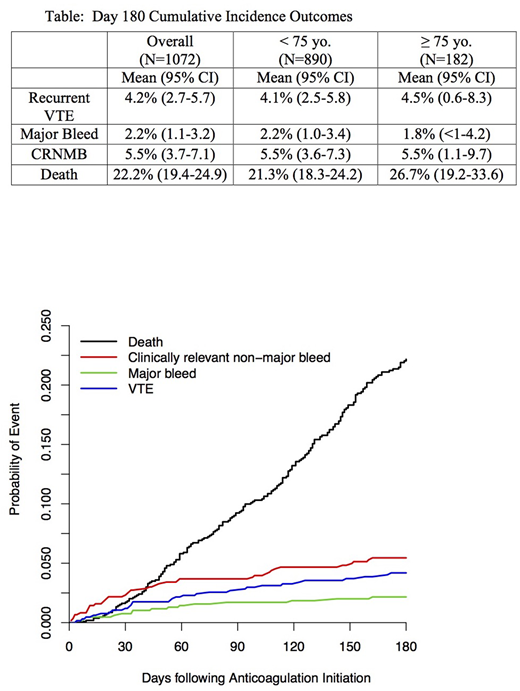
Results: At 6 months, the cumulative incidence for the various endpoints estimated within a competing risks framework were; recurrent VTE (4.2%), MB (2.2%), CRNMB (5.5%). Overall, the 6-month incidence of death was 22.2%. In the elderly patients, the risks of recurrent VTE and bleeding were similar to the <75 yo patients. It should be noted that only approximately half (48%) the elderly patients received reduced-dose Riva, at the discretion of the treating physician, and the numbers were too small to allow for comparison of full-dose and reduced dose.
Conclusions: In our expanded experience of Riva therapy for CAT, applying our CP, we continue to maintain low rates of recurrent VTE and bleeding. Allowing for differences in methodology between a cohort study and randomized clinical trials, the rate of recurrent VTE was as low as the DOAC arm in Hokusai VTE Cancer and Select-D studies. Further, by applying the exclusion criteria in our CP, and not treating patients with known GI/GU lesions, we achieved a low rate of bleeding compared with the DOAC treatment arms in the two recent randomized clinical trials. Those two trials demonstrated bleeding rates greater than LMWH, particularly GI/GU bleeds. We saw no increased rates of recurrent VTE or bleeding in the elderly, which is reassuring, but we cannot conclude if reduced dose is of benefit. These new expanded observations further support the validity of our CP.
The key to anticoagulation choice for CAT is not which anticoagulant is "better," but rather which anticoagulant to choose for a specific patient. In the absence of GI/GU contraindications, Riva provides effective and safe anticoagulation, at substantially lower cost and burden to the patient than LMWH. In contrast, we propose that LMWH is preferable in patients with GI/GU lesions. (We are now obtaining specific data for that subgroup).
Soff:Amgen: Research Funding; Janssen: Research Funding. Mantha:Heidell, Pittoni, Murphy & Bach, LLP: Consultancy; GLG: Consultancy; Janssen: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal